



Dark spots frustrate people more than wrinkles, and uneven tone consistently ranks among the most common skin concerns across ages, skin types, and backgrounds. Hyperpigmentation feels especially discouraging because it lingers long after the original trigger fades. Acne clears, but the mark stays. A sunny vacation ends, yet discoloration remains visible for months. This disconnect between cause and resolution fuels confusion, impatience, and misuse of treatments.
Hyperpigmentation Recommended Products





Understanding skin hyperpigmentation pathways matters because pigment does not behave randomly. Melanin production follows specific biological signals tied to protection, inflammation, and repair. When those signals remain active longer than needed, discoloration becomes persistent rather than temporary. Once this process becomes clear, treatment decisions become safer, more targeted, and far more realistic.

What hyperpigmentation is and why skin produces pigment
Skin color comes from melanin, a pigment produced by specialized cells called melanocytes. These cells live in the basal layer of the epidermis and function as part of the skin’s defense system. When skin encounters stress such as ultraviolet exposure, inflammation, heat, friction, or injury, melanocytes respond by increasing melanin production. That pigment absorbs and disperses energy that might otherwise damage DNA and cellular structures.
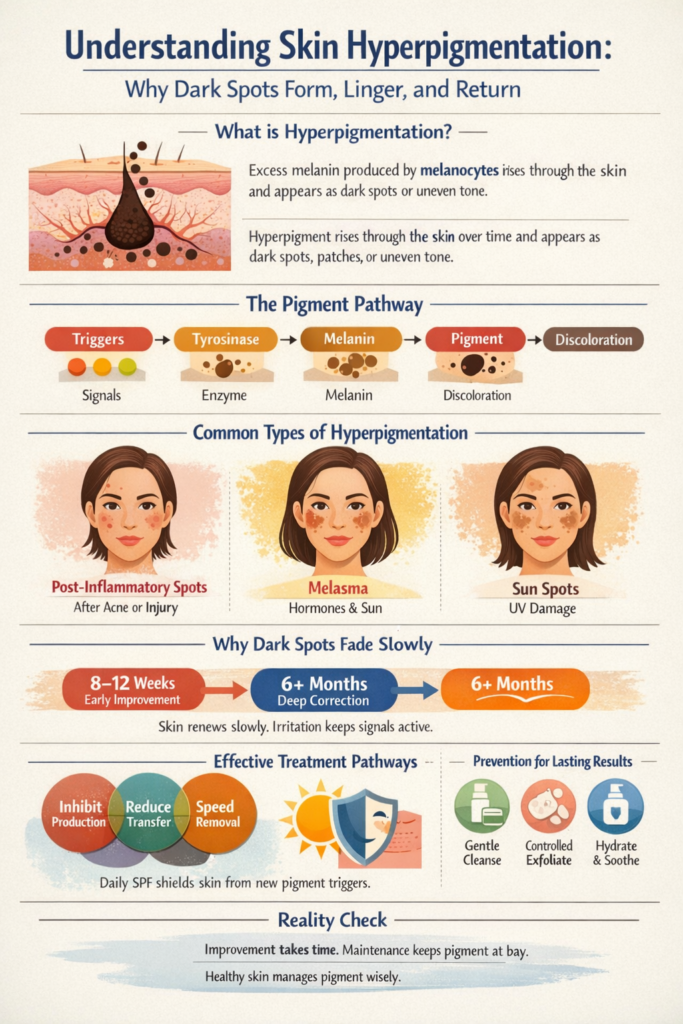
Hyperpigmentation occurs when this protective response overshoots or fails to shut off. Excess melanin accumulates in localized areas, forming dark spots, patches, or uneven tone. The appearance depends largely on depth, with superficial pigment appearing tan or brown and deeper pigment taking on gray or bluish tones. The deeper pigment settles, the longer it takes to fade.
Melanin itself is not harmful, nor is it a flaw. It protects skin and supports long-term resilience. Problems arise only when pigment production becomes chronic rather than situational. In those cases, skin continues defending against a threat that no longer exists.
How pigment pathways work beneath the surface
Pigment formation begins with tyrosine, an amino acid present in skin cells. Through a series of enzymatic reactions, tyrosine converts into melanin. The primary enzyme driving this process is tyrosinase, which largely determines how much pigment is produced. When tyrosinase activity increases, melanin output rises accordingly.
Several triggers influence this pathway. Ultraviolet radiation remains the most powerful, activating melanocyte-stimulating signals and increasing oxidative stress. Inflammation sends similar signals through cytokines and prostaglandins, even when skin does not appear visibly irritated. Mechanical trauma such as aggressive exfoliation or repeated friction can activate melanocytes in the same way.
Ultraviolet radiation remains the most powerful, activating melanocyte-stimulating signals and increasing oxidative stress.
Hormones further complicate pigment behavior. Estrogen and progesterone increase melanocyte sensitivity, which explains why melasma commonly appears during pregnancy or with hormonal medications. Heat and visible light also stimulate pigment cells, particularly in medium to deep skin tones. These layered signals explain why some discoloration proves so persistent.
Once melanin forms, it packages into melanosomes and transfers into surrounding skin cells. As surface cells migrate upward and shed, pigment should gradually fade. Hyperpigmentation develops when production outpaces removal or when melanin settles deeper into the skin structure.

Common causes that keep pigment active
Sun exposure remains the most common driver of hyperpigmentation. Ultraviolet radiation repeatedly stimulates melanocytes, especially in areas exposed daily such as the face, chest, and hands. Over time, this repeated stimulation leads to uneven tone and visible spots. Even brief daily exposure accumulates and reinforces pigment signals.
Hormonal shifts also play a significant role in hyperpigmentation. Melasma often develops during pregnancy or with hormonal contraceptive use and appears as symmetrical facial patches. These patches tend to involve deeper pigment, making them slower to respond and more likely to recur. Hormonal influence explains why some discoloration persists despite careful topical care.
Inflammation activates another pathway. Acne, eczema, insect bites, cosmetic procedures, and rashes can all trigger post-inflammatory hyperpigmentation. The skin heals structurally, but pigment production remains elevated at the injury site. This response reflects the skin’s attempt to protect itself during repair.

Heat and visible light also contribute to hyperpigmentation. These triggers stimulate melanocytes through pathways separate from ultraviolet radiation. This effect proves especially relevant for medium to deep skin tones. Discoloration may persist even with diligent sunscreen use if heat and visible light exposure remain unaddressed.
Genetic predisposition influences how easily pigment activates and how long it persists. Some skin types produce melanin more readily or retain pigment longer after triggers resolve. Genetics do not make hyperpigmentation inevitable, but they shape response patterns. Understanding predisposition helps set realistic expectations.
Different types of hyperpigmentation and how they behave
Post-inflammatory hyperpigmentation develops after visible inflammation or injury and appears as flat brown or gray marks. Melasma presents as symmetrical facial patches driven by hormonal and environmental signals. Sunspots reflect cumulative UV exposure over many years. Each behaves differently because pigment depth and signaling differ.
Freckles behave differently from other forms of hyperpigmentation. They reflect localized increases in melanin without an increase in melanocyte number. Freckles darken with sun exposure and fade when exposure decreases. They are genetically influenced, benign, and typically do not require treatment.
Age spots and how hyperpigmentation behaves in mature skin
Age spots, sometimes called liver spots, are flat brown or tan patches that develop after years of repeated sun exposure. The correct medical term is solar lentigines, and despite the common name, they have no connection to liver health. These spots form when melanocytes become chronically overstimulated by ultraviolet radiation over decades rather than weeks or months. They most often appear on the face, hands, chest, shoulders, and arms, where sun exposure accumulates over time.

Mature skin handles pigment differently than younger skin. Cell turnover slows with age, which means pigmented cells remain visible longer before shedding. The epidermis thins, reducing the margin for aggressive exfoliation and increasing irritation risk. Inflammation also resolves more slowly, which can quietly reactivate pigment pathways even when skin appears calm.
Age spots tend to be more stable than post-inflammatory hyperpigmentation, but they are also more resistant to rapid change. They respond best to long-term pigment regulation combined with consistent sun protection rather than short bursts of aggressive treatment. Improvements often appear gradually as edges soften and tone becomes more even rather than spots disappearing completely.
Managing hyperpigmentation in mature skin requires different expectations and pacing. Gentle exfoliation supports renewal without provoking inflammation. Pigment-regulating ingredients work best when paired with barrier support and antioxidant protection. Results take longer, but they are often more durable when skin is allowed to respond at its own pace.

Why pigment fades slowly and patience matters
Skin renewal follows a biological timeline that cannot be rushed. In younger skin, the epidermis renews roughly every four to six weeks, and that process slows with age. Surface pigment clears first as pigmented cells shed naturally. Deeper pigment must migrate upward before fading becomes visible.
Early improvement often reflects improved light reflection rather than full correction. Meaningful change for stubborn discoloration often appears around the six-month mark when care remains consistent and gentle. Expecting rapid change often leads to overtreatment. Patience protects progress.
Treatment pathways that work together
Effective pigment care targets multiple steps in the hyperpigmentation process rather than relying on a single ingredient or mechanism. Some topical ingredients work upstream by reducing melanin production, primarily by calming tyrosinase activity within melanocytes. Others act downstream by limiting how much pigment transfers into surface skin cells. Still others focus on clearing pigment that has already formed by supporting steady cell turnover.
Ingredients that reduce melanin production tend to work gradually and require consistent use. Azelaic acid, kojic acid, arbutin, and certain vitamin C derivatives help regulate tyrosinase activity and oxidative signaling within pigment cells. These ingredients typically begin to influence pigment behavior within eight to twelve weeks, though visible fading often continues for several months. Their strength lies in prevention and signal control rather than rapid surface change.
Ingredients that limit pigment transfer focus on interrupting how melanin moves from melanocytes into surrounding skin cells. Niacinamide is one of the most studied examples and works best when used consistently over time rather than aggressively. Results usually become noticeable within eight to ten weeks as new pigment formation slows. These ingredients support even tone without increasing irritation risk.
Glycolic acid, lactic acid, and gentle enzymatic exfoliants help remove pigmented cells more efficiently as skin renews itself.
Exfoliating acids address pigment already present in the upper layers of skin. Glycolic acid, lactic acid, and gentle enzymatic exfoliants help remove pigmented cells more efficiently as skin renews itself. Early brightening from exfoliation can appear within four to six weeks, but this reflects surface clearing rather than true pigment correction. Used thoughtfully, exfoliants enhance the results of pigment regulators rather than replacing them.
Antioxidants play a supporting but essential role in pigment management. Vitamin C, resveratrol, green tea, and similar compounds reduce oxidative stress that fuels melanocyte activation. Their benefits build gradually and become more apparent over two to three months of regular use. Antioxidants help stabilize results and reduce the chance of rebound pigmentation when skin faces environmental stress.
Barrier-supportive ingredients complete the system. Ceramides, fatty acids, soothing botanical extracts, and humectants reduce inflammation and help skin tolerate active treatments. This support lowers the likelihood of irritation-driven pigment relapse. Skin that feels comfortable and resilient responds more predictably to brightening strategies.
The most effective topical combinations respect timing and tolerance. A pigment regulator paired with a pigment transfer inhibitor addresses new discoloration, while gentle exfoliation supports clearance of existing spots. Antioxidants and barrier support allow these actives to work without triggering defensive pigment responses. Results improve when this balance is maintained consistently over months rather than pushed aggressively for weeks.
Pigment correction rewards patience because it follows skin biology, not marketing timelines. Most topical routines show early improvement within two to three months, with deeper or hormonally influenced discoloration requiring six months or longer. No combination overrides the need for sun protection and inflammation control. When pathways work together, progress becomes steadier, safer, and far more durable.

Why aggressive treatments and DIY misuse backfire
Overtreatment remains one of the most common reasons hyperpigmentation worsens. High-strength acids, excessive exfoliation, and frequent procedure stacking create inflammation even without visible irritation. That inflammation reactivates melanocytes and leads to rebound discoloration. More effort often produces less progress.
DIY misuse creates similar problems. Mixing actives without understanding concentration or frequency increases irritation risk. Even natural ingredients trigger pigment when used incorrectly. Skin responds to stress, not intent.
When professional diagnosis matters
Not all discoloration behaves the same way, and not all dark spots are benign. A dermatologist can assess pigment depth, distribution, and triggers through clinical examination. Tools such as dermoscopy help differentiate pigment patterns. In rare cases, biopsy confirms diagnosis.
Professional evaluation matters when discoloration appears suddenly, changes rapidly, or resists consistent care. Irregular borders or texture changes also warrant assessment. Proper diagnosis reduces risk and improves outcomes.
Sun protection as the deciding factor
Sun exposure undermines every pigment treatment. Ultraviolet radiation, visible light, and heat stimulate melanocytes even on cloudy days. Without daily protection, new pigment forms while old pigment fades. Protection determines success.
Prevention and maintenance shape long-term results
Preventing hyperpigmentation means reducing triggers before pigment pathways activate. Gentle cleansing preserves barrier health. Controlled exfoliation avoids inflammation. Hydration and calming care reduce reactivity. Maintenance keeps pigment signals quiet.
Living with pigment without letting it define skin health
Hyperpigmentation reflects biology responding to stress, not neglect or failure. Improvement often means softer edges and fewer new spots rather than total erasure. Healthy skin functions better even when faint discoloration remains. Balance supports resilience.

Frequently asked questions about hyperpigmentation
How long does it take to see visible improvement in dark spots and uneven tone?
Pigment correction follows the pace of skin renewal, not the pace of marketing claims. Most routines show early tone softening around the eight-to-twelve-week mark when use stays consistent and irritation stays low. This stage reflects surface pigment clearing and better light reflection rather than full correction. Deeper pigment sits lower in the skin and clears more slowly as those cells move upward over time. Six months often marks meaningful improvement for stubborn discoloration, especially melasma or long-standing sun damage. Progress continues beyond that point when protection and maintenance stay in place.
Is it safe and effective to combine brightening ingredients with exfoliating acids?
Combining actives works best when structure replaces enthusiasm. Brighteners target pigment production and transfer, while exfoliants help remove already pigmented cells from the surface. When both work together in a controlled routine, results improve steadily. Problems start when exfoliation outpaces skin recovery and triggers inflammation. Adding one active at a time allows skin to adapt without stress signals flaring. Calm, comfortable skin responds better to pigment correction than skin pushed into constant repair mode.
Do dark spots come back after they fade?
Hyperpigmentation returns when the original triggers return. Sun exposure remains the most common driver, followed by inflammation and hormonal shifts. Skin cells remember stress, so repeated exposure trains melanocytes to respond faster and more intensely. Maintenance routines exist to keep those signals quiet rather than erase them entirely. Daily protection, gentle care, and continued use of supportive ingredients reduce how often spots reappear and how dark they become. Long-term consistency shapes long-term stability.
Why does pigment correction demand so much patience?
Skin prioritizes protection over aesthetics, and pigment forms as part of that defense system. When skin senses threat, it responds first and asks questions later. Reversing that response takes time because signaling pathways need repeated reassurance before they quiet down. Aggressive treatment often slows progress by keeping those alarms active. Supportive care allows skin to feel safe enough to reset its behavior. Patience rewards effort with steadier, more durable improvement rather than short-lived change.
References
- Tyrosinase is a key, rate-limiting enzyme in melanin synthesis – https://pmc.ncbi.nlm.nih.gov/articles/PMC6010116/
- Tyrosinase as the rate-limiting enzyme in melanin biosynthesis, overview of regulation – https://www.sciencedirect.com/science/article/pii/S0022202X15355573
- Niacinamide reduces pigmentation by inhibiting melanosome transfer (melanocyte to keratinocyte) – https://pubmed.ncbi.nlm.nih.gov/12100180/
- Post-inflammatory hyperpigmentation mechanism, excess melanin after inflammation, epidermal transfer details – https://pmc.ncbi.nlm.nih.gov/articles/PMC2921758/
- Post-inflammatory hyperpigmentation clinical overview, triggers, epidermal vs dermal deposition – https://www.ncbi.nlm.nih.gov/books/NBK559150/
- Melasma pathogenesis review, multifactorial drivers including solar radiation and hormones – https://pmc.ncbi.nlm.nih.gov/articles/PMC9464278/
- Visible light and UVA1 role in melasma, plus a commonly cited prevalence range in certain populations – https://pmc.ncbi.nlm.nih.gov/articles/PMC9790748/
- Focused review on PIH pathophysiology (peer-reviewed dermatology journal) – https://onlinelibrary.wiley.com/doi/full/10.1111/pcmr.13038



